Time: 0 second
Chest X-ray
5-days post-operatively you review the patient who is being treated for a wound infection. A wound swab has been sent for culture and has grown MRSA

Question No. 3
Q: What is the most obvious abnormality on the chest x-ray?
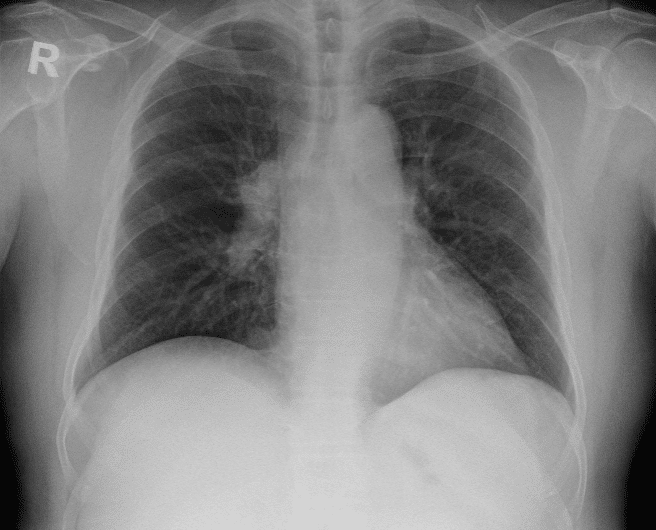
Answer No. 3
A right-sided hilar mass is present
Question No. 8
Q: How would you assess her fitness for lung resection?
Answer No. 8
- BTS recommends a tripartite risk assessment model when assessing fitness for lung resection surgery including:
- Risk of operative mortality
- Risk of perioperative myocardial events
- Risk of postoperative dyspnoea
- These can be used to discuss individual risks with the patient and MDT

