Time: 0 second
Question No. 9
Q: What are the electrocardiographic (ECG) findings seen in PE?
Answer No. 9
- ECG findings are also variable and neither sensitive or specific
- A normal ECG is seen in up to 18% of cases
- Abnormalities seen include:
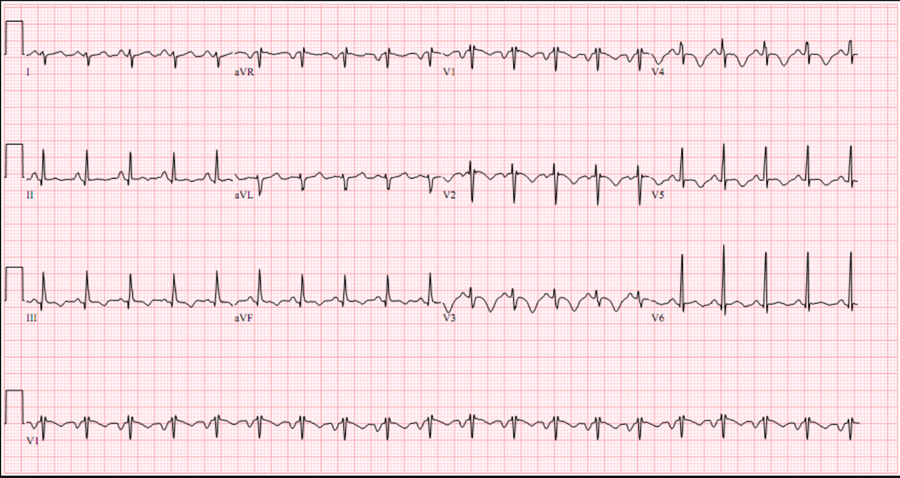
- Sinus tachycardia (most common - 44%)
- Atrial arrhythmias (most frequently atrial fibrillation)
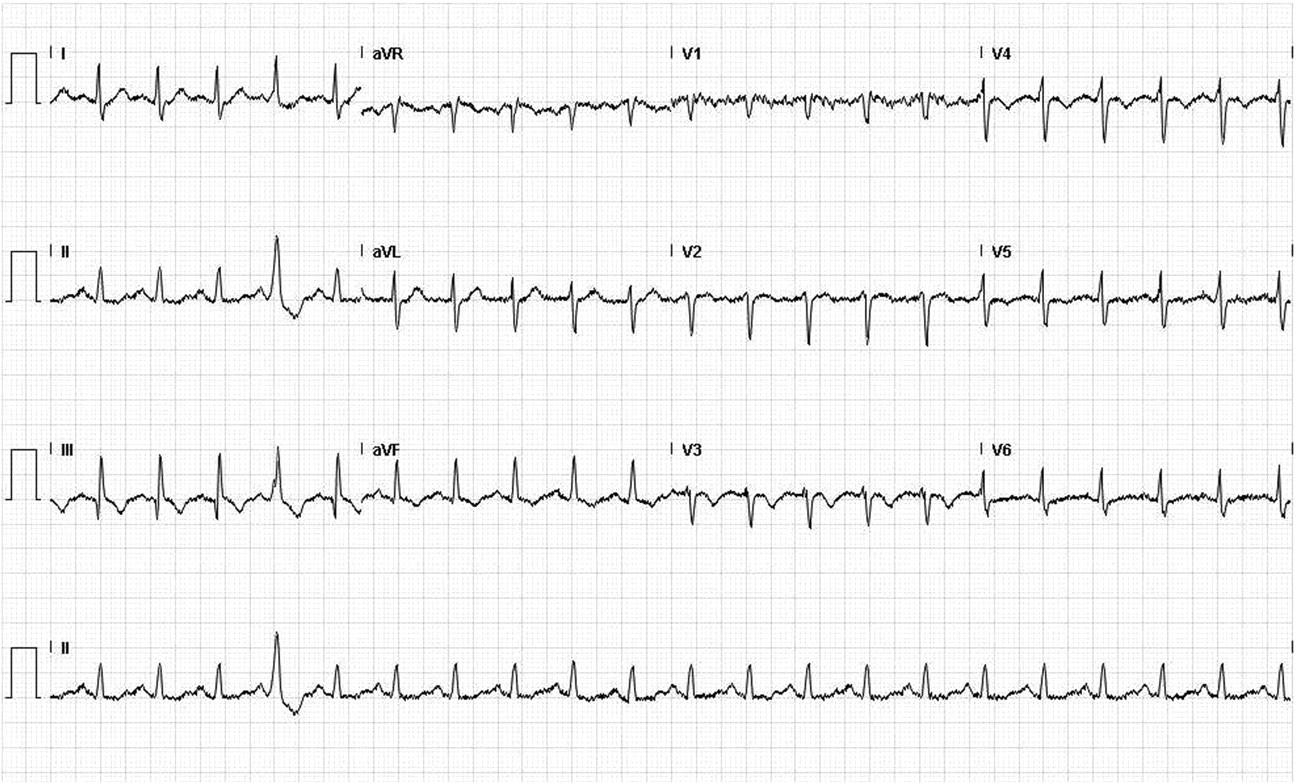
- Classic S1Q3T3 (10%)
- Deep S-wave in lead I, Q-wave in III and an inverted T-wave in III
- Complete or incomplete right bundle branch block (15%): rSR’ in V1
- Associated with increased mortality
- Acute right ventricular strain (34%)
- T-wave inversion in the right precordial leads (V1-4) and the inferior leads (II, III, aVF)
Associated with high pulmonary artery pressures
- T-wave inversion in the right precordial leads (V1-4) and the inferior leads (II, III, aVF)
- Right axis deviation (15%):
- May be extreme deviation - between 0 and -90°
- Non-specific ST-segment and T-wave changes:
- ST-elevation and depression
- T-wave inversion

Question No. 11
Q: Why do pulmonary emboli cause haemodynamic instability?
Answer No. 11
- PE can lead to right ventricular (RV) failure due to acute pressure overload:
- Pulmonary artery pressure (PAP) increases in the presence of obstruction
- Becomes evident if >30-50% of the total cross-sectional occluded by thromboemboli
- Obstruction due to:
- Mechanical obstruction from clot burden
- Vasoconstriction, mediated by the release of thromboxane A2 and serotonin
- Results in increased RV afterload and subsequent dilatation:
- Initial compensation occurs via Frank Starling mechanism with increased myocyte stretch
- Neurohumoral activation leads to inotropic and chronotropic stimulation.
- RV adaptation is limited and is unable to generate a mean PAP >40 mmHg
- Ventricle non-preconditioned and thin-walled
- Enters cycle of progressive RV failure with imbalanced oxygen supply / demand and decreased contractility
- Progressive impact on left ventricle (LV) and systemic circulation:
- Bowing of intraventricular septum impairs LV filling
- Further exacerbated by development of right bundle branch block
- Leads to reduced cardiac output and systemic hypotension
- Exacerbates impaired coronary driving pressure to the overloaded RV and further imbalances myocardial oxygen supply and demand
- May be a secondary inflammatory response due to massive neurohumoral activation

Question No. 12
Q: How would your diagnostic strategy change now the patient is demonstrating haemodynamic instability?
Answer No. 12

Question No. 13
Q: What are the echocardiographic findings seen in PE?
Answer No. 13
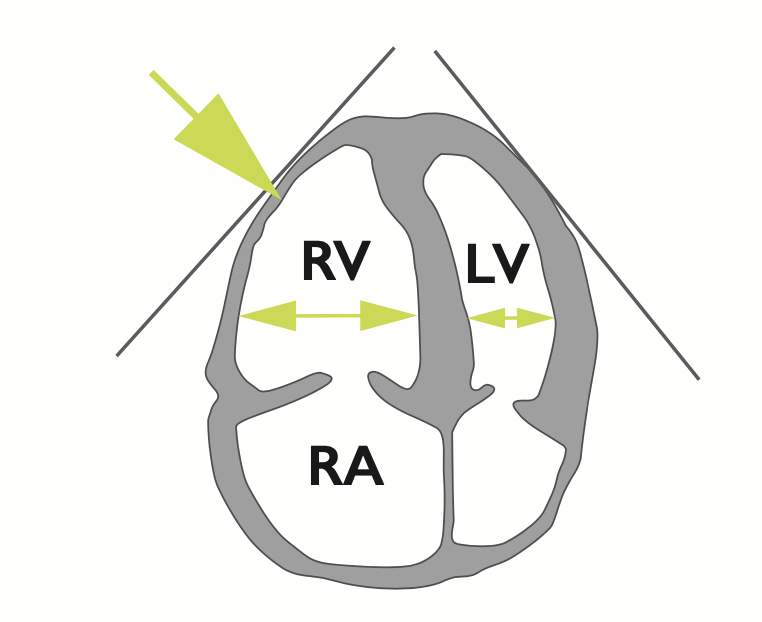
- Dilatation of the right ventricle
- Impaired right ventricular function
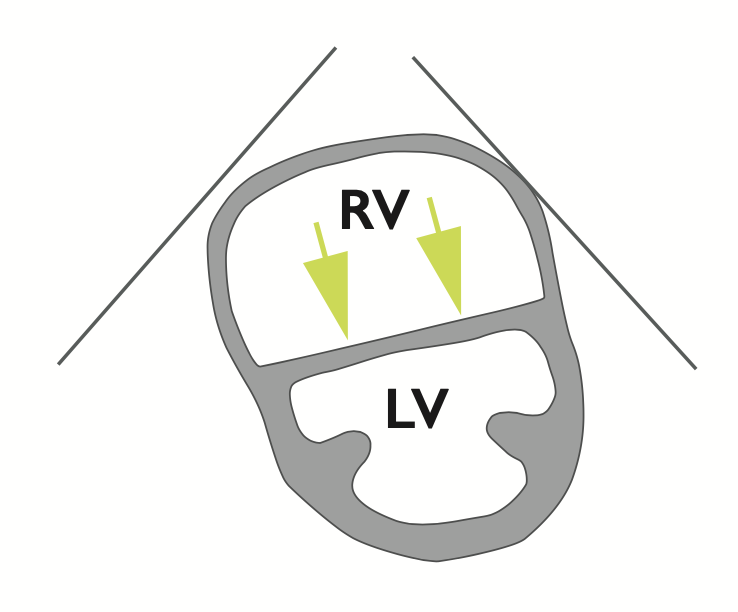
- Flattened intraventricular septum
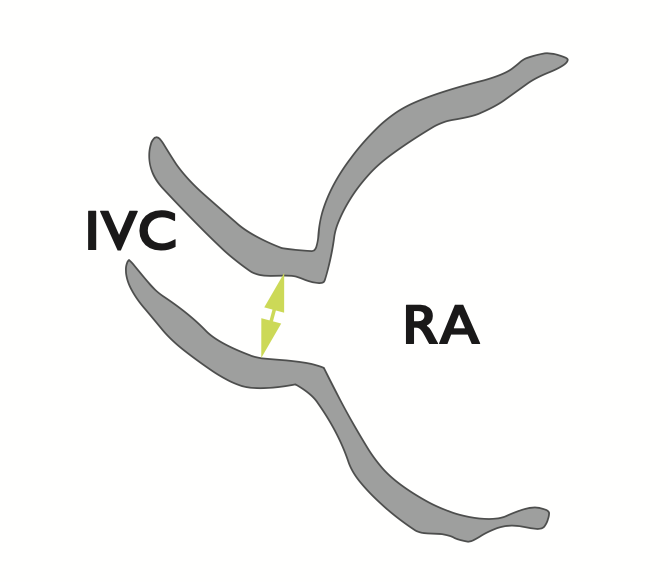
- Distended inferior vena cava with diminished inspiratory collapsibility
- Tricuspid regurgitation
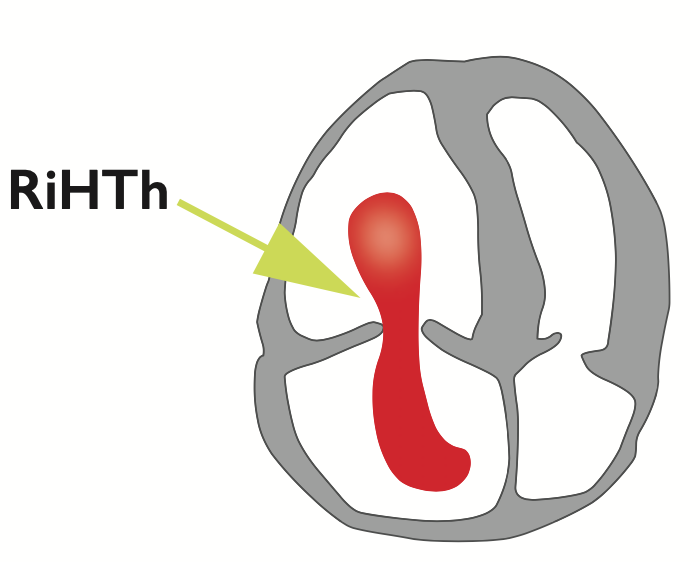
- Mobile thrombus in the right heart