Time: 0 second
Case Information
This ECG has been done 30 minutes ago…

Question No. 3
Q: What does the ECG show? (2 marks)
Answer No. 3
- Incomplete RBBB 1 (rSR’ in V1)
- T wave inversion in V1-V3 1 (mimics anterior ischemia)
- Sinus tachycardia 1
2
Question No. 9
Q: Other than impaired right ventricular function what abnormal features on a transthoracic echocardiogram would support a diagnosis of PE? (3 marks)
Answer No. 9
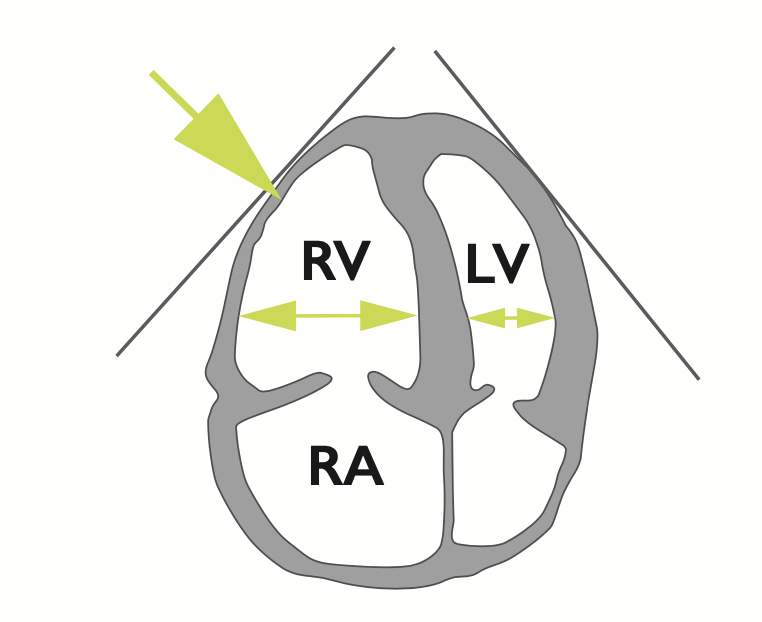
- Dilatation of the right ventricle 1
- Impaired right ventricular function
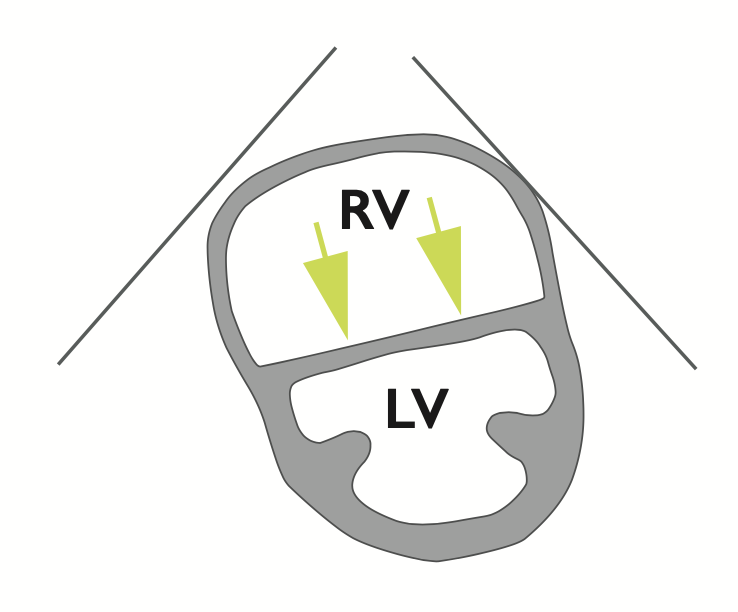
- Flattened intraventricular septum 1
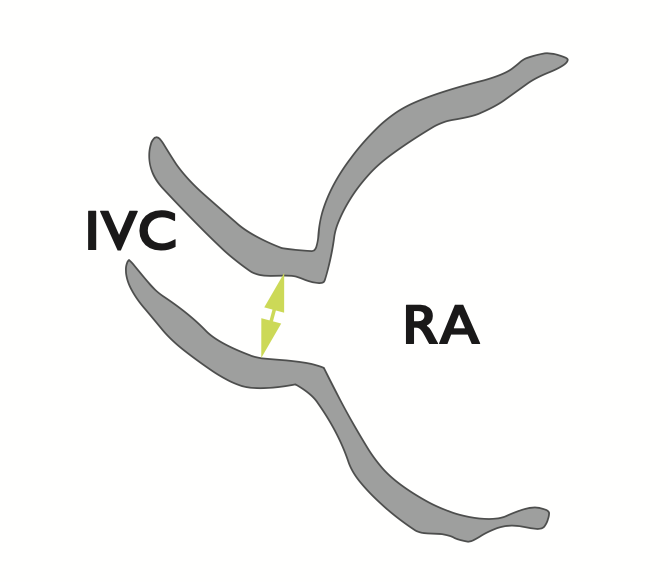
- Distended inferior vena cava with diminished inspiratory collapsibility 1
- Tricuspid regurgitation 1
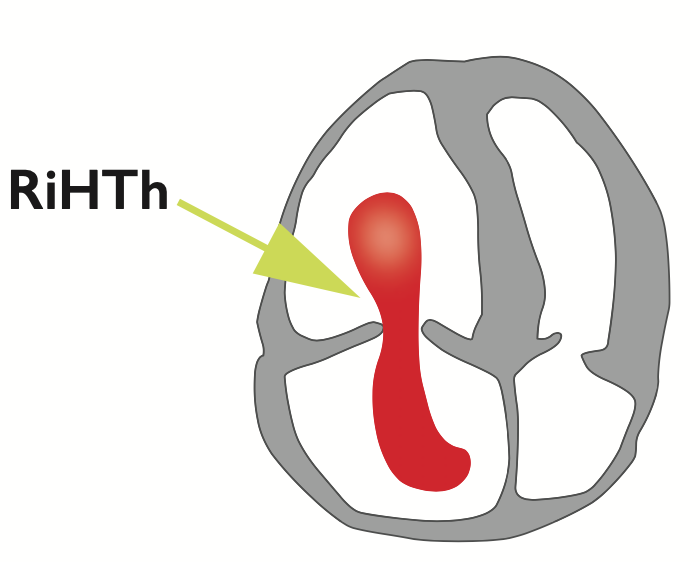
- Mobile thrombus in the right heart 1

3